Source: Canva
What, Exactly, is Burnout?
Burnout is a psychological symptom that results from chronic work-related stress (Melamed et al., 2006). Melamed et al. define burnout simply as “emotional exhaustion, physical fatigue, and cognitive weariness.”[1] Specifically, Maslach et al. find that burnout can be conceptualized along three dimensions:[2,3]
Exhaustion - stress and chronic fatigue due to overwhelming demands.
Cynicism - apathy, loss of interest in work, and a sense of futility and meaninglessness toward one’s job.
A decrease in quality of work performance - the manifestation of reduced feelings of performance-effectiveness or accomplishment
The multivariate impact of burnout is quantifiable. Burnout negatively impacts productivity and can be measured by: quantity of sick leave days, job retention, and the intention to change jobs.[4] Studies have also found higher levels of burnout have correlated with increased inflammation biomarkers, risk of cardiovascular disease, sleep disturbances, fatigue, and mood disturbances.[5-8]
How Does Burnout Arise?
In addition to more obvious factors like an overwhelming workload, two decades of research on burnout have illuminated some lesser known factors that influence one’s likelihood of burning out. If people perceive that they have the capacity to influence decisions within their workplace and believe they have access to resources necessary to perform well, job engagement is likely to increase. When people feel insufficient recognition or reward (i.e. financial, social, institutional) for their work, both they (as individuals) and their work can feel devalued; this is found to be closely related to feelings of inefficacy and decreased satisfaction. Interpersonal dynamics within the workplace also affect one’s experience of burnout; relationships characterized by support and trust protect against burnout, while unresolved conflict and a lack of trust between peers or coworkers are correlated with greater burnout risk. Fair and equitable policies are also important, as people who feel that they are not being appropriately respected can become chronically cynical, angry, or hostile. Finally, a conflict of values between an individual and their organization can increase one’s likelihood of developing burnout, as the continual pressure to make trade-offs between their values and obligations can affect stress and exhaustion levels.[9]
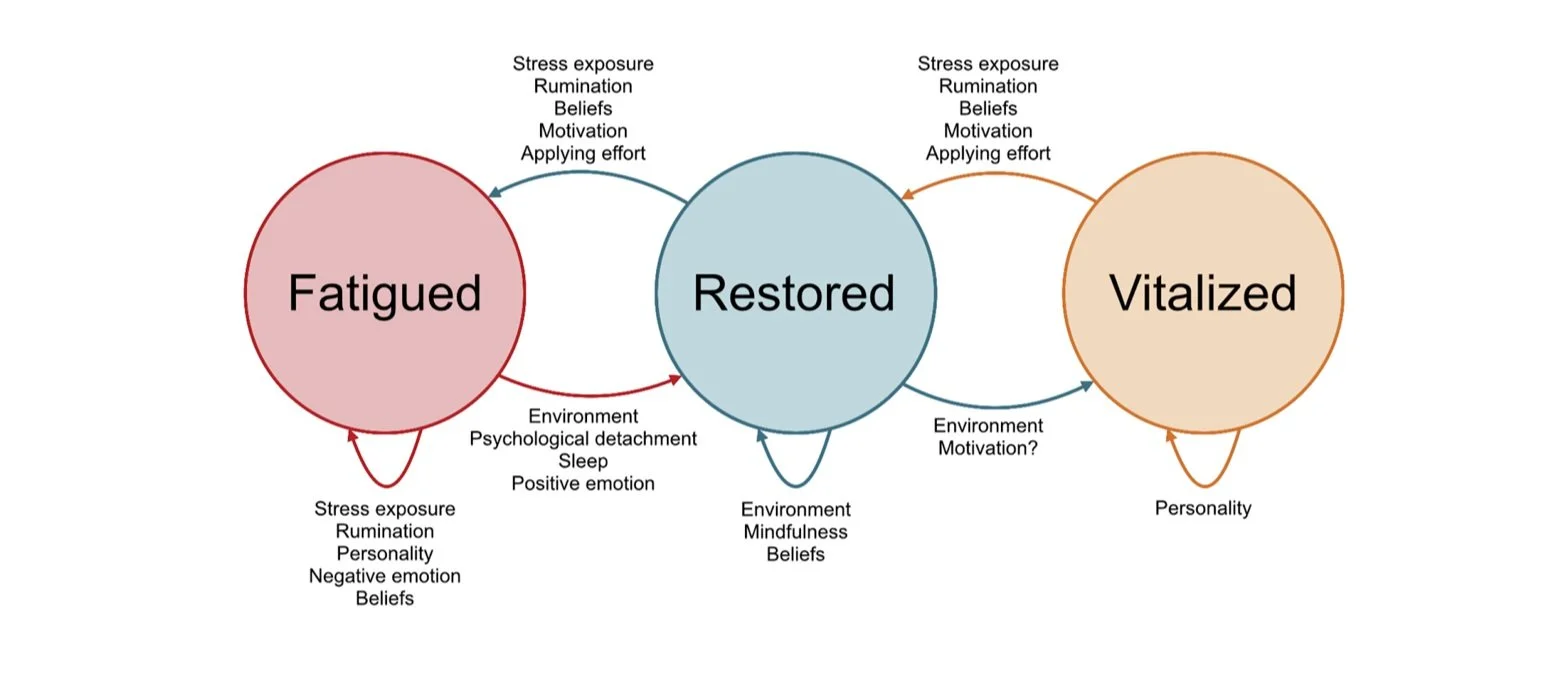
Figure 1: List of possible burnout symptoms

Image based on a list produced by Schaufeli & Enzmann (1998) [10]
Who Burns Out the Quickest?
Different individuals working under the same job conditions will not necessarily feel burned out at the same time or to the same degree. This is because burnout is a response to stress and individuals evaluate, cope with, and respond to stressors differently. One study by Ghorpade et al. (2007) finds that differences in personality can influence whether one conserves resources (consequently protecting themselves) or becomes susceptible to stressors. Further, extroversion and emotional stability have been found to be negatively related to emotional exhaustion.[11] Openness and agreeableness are also negatively correlated with burnout, while conscientiousness and neuroticism appear to be positively associated.[12,13]
Something that researchers have struggled to account for is how often burnout might be mislabeled as depression or anxiety, and how such misdiagnoses can lead to ineffective treatment interventions. People suffering from burnout might appear to be depressed, as the symptoms of burnout resemble those of depression (e.g. loss of interest, fatigue, impaired concentration, depressed mood).[14] As there are no diagnostic criteria for burnout and it is not mentioned in the DSM-5, one cannot be formally diagnosed with the condition. One major distinction between depression and burnout is that burnout arises specifically in work-related contexts whereas depression is pervasive across different contexts.[15]
Burnout from Online and Telecommunication-Based Environments
It is often contended that screen time is associated with copious amounts of stress-related symptoms, including psychological, cognitive, and muscular impairments.[16,17] Mheidly et al. (2020) write that pandemics “are often associated with a state of stress and panic. Accordingly, strain resulting from telecommunication can accumulate with other stressors to lead to exhaustion, anxiety, and burnout.”[18] They note that imposed lockdowns, quarantines, and the inability to socialize as a result of the COVID-19 pandemic have led to considerable disruptions in lives, often accompanied by increased tension, anxiety, boredom, and disturbed sleep cycles. Within workplaces, promotions have been delayed and wages have been cut; these negative changes can create adverse levels of pressure and anxiety within people.
Mheidly et al. (2020) recommend promoting awareness regarding stress and burnout as a result of increased telecommunication. They note the following measures are likely to combat this type of burnout: increasing the frequency of breaks between virtual lectures and teleconferences to both reduce eye strain and prevent attention loss, increasing podcast-based communication as a substitute for visual screen time, and implementing healthy practices throughout the work or school day. Yoga, in particular, has received growing research attention, with evidence indicating it can be an effective intervention to reduce stress, increase physical activity, and improve well-being.[19-21]
How to Recover from Burnout
Just as the onset and development of burnout change depending on the individual, so too does the recovery. While Heng & Schabram (2021) believe that the best cure for burnout is prevention altogether, that isn’t always realistic. Therefore, they emphasize the importance of agency in the restoration process. Their research finds that to “effectively overcome burnout, employees must feel empowered to take control over their own lives and decisions.” Rather than expect or request a manager to intervene and improve coworker relations, they note that it is more effective for employees to reaffirm their own social networks. In a subsequent study where they surveyed social service workers (people prone to chronic burnout), Heng & Schabram found “those who were already suffering from burnout had a harder time engaging in acts of self- or other-care, [while] those who were able to muster the energy to practice compassion showed significant reductions in burnout.”[22] Other research has found that mindfulness practices such as breathing exercises, gratitude exercises, yoga, and movement can be effective at cultivating compassion, and that compassion meditation training can rewire neural circuitry in the brain.[23,24]
Self-care and healthy practices are crucial to implement for burnout recovery. Such practices can include:
stretching to mitigate tension brought on by extended sitting
practicing agency and taking control in areas of work or school where one can make changes for themselves
reflecting on one’s support system and building relationships where trust and respect are foundational
engaging in self-compassion
It’s also important to be aware that the symptoms of burnout can resemble those of depression; if one’s cynicism and exhaustion begin to pervade other areas of life besides work, then different approaches (e.g., therapy or medication) may be more effective or necessary for healing to occur.
For more information, click here to access an interview with SAS Therapist, Jim McDonnell, on high-stress employment.
Contributed by: Maya Hsu
Editor: Jennifer (Ghahari) Smith, Ph.D.
References
1 Melamed, S., Shirom, A., Toker, S., Berliner, S., & Shapira, I. (2006). Burnout and risk of cardiovascular disease: Evidence, possible causal paths, and promising research directions. Psychological Bulletin, 132(3), 327–353. https://doi.org/10.1037/0033-2909.132.3.327
2 Maslach, C., Jackson, S. E., & Leiter, M. P. (1997). Maslach Burnout Inventory: Third edition. In C. P. Zalaquett & R. J. Wood (Eds.), Evaluating stress: A book of resources (pp. 191–218). Scarecrow Education.
3 Koutsimani, P., Montgomery, A., & Georganta, K. (2019). The Relationship Between Burnout, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Frontiers in psychology, 10, 284. https://doi.org/10.3389/fpsyg.2019.00284
4 Storm, K., & Rothmann, S. (2003). The relationship between burnout, personality traits and coping strategies in a corporate pharmaceutical group. South African Journal of Industrial Psychology, 29(4), 35-42. Retrieved from https://www.researchgate.net/publication/47739448_The_relationship_between_b urnout_personality_traits_and_coping_strategies_in_a_corporate_pharmaceutical _group
5 Toker, S., Shirom, A., Shapira, I., Berliner, S., & Melamed, S. (2005). The association between burnout, depression, anxiety, and inflammation biomarkers: C-reactive protein and fibrinogen in men and women. Journal of Occupational Health Psychology, 10(4), 344-362. http://dx.doi.org/10.1037/1076-8998.10.4.344
6 Toppinen-Tanner, S., Ahola, K., Koskinen, A., & Vaananen, A. (2009). Burnout predicts hospitalization for mental and cardiovascular disorders: 10 - year prospective results from industrial sector. Stress and Health, 25(4), 287-296. http://dx.doi.org/10.1002/smi.1282
7 Rosen, I. M., Gimotty, P. A., Shea, J. A., & Bellini, L. M. (2006). Evolution of sleep quantity, sleep deprivation, mood disturbances, empathy, and burnout 39 among interns. Academic Medicine, 81(1), 82-85. Retrieved from http://journals.lww.com/academicmedicine/Fulltext/2006/01000/Evolution_of_Sl eep_Quantity,_Sleep_Deprivation,.20.aspx
8 Ahola, K., Honkonen, T., Kivimäki, M., Virtanen, M., Isometsä, E., Aromaa, A., & Lönnqvist, J. (2006). Contribution of burnout to the association between job strain and depression: The Health 2000 Study. Journal of Occupational and Environmental Medicine, 48(10), 1023-1030. http://dx.doi.org/10.1097/01.jom.0000237437.84513.92
9 Maslach, C., & Leiter, M. P. (2016). Understanding the burnout experience: Recent research and its implications for psychiatry. World psychiatry : official journal of the World Psychiatric Association (WPA). Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4911781/#wps20311-bib-0024
10 Schaufeli, W., & Enzmann, D. (1998). The burnout companion to study and practice: A critical analysis. Taylor & Francis.
11 Ghorpade, J., Lackritz, J., & Singh, G. (2007). Burnout and personality. Journal of Career Assessment, 15(2), 240–256. https://doi.org/10.1177/1069072706298156
12 Anvari, M. R., Kalali, N. S., & Gholipour, A. (2011). How does personality affect on job burnout? International Journal of Trade, Economics and Finance, 2(2), 115-119. Retrieved from http://www.ijtef.org/papers/88-F00068.pdf
13 Dargah, H. G., & Estalkhbijari, Z. P. (2012). The relationship between the Big Five Personality Factors and job burnout. International Journal of Asian Social Science, 2(11), 1842-1850. Retrieved from http://www.aessweb.com/pdffiles/ijass%20pp.1842-1850.pdf
14 American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). Washington, DC: American Psychiatric Pub.
15 Iacovides, A., et al. (2003). The relationship between job stress, burnout and clinical depression. Journal of Affective Disorders, 75(3), 209-221. https://doi.org/10.1016/S0165-0327(02)00101-5
16 Lemola, S., Perkinson-Gloor, N., Brand, S., Dewald-Kaufmann, J. F., & Grob, A. (2014). Adolescents' electronic media use at night, sleep disturbance, and depressive symptoms in the smartphone age - Journal of Youth and adolescence. SpringerLink. Retrieved January from https://link.springer.com/article/10.1007/s10964-014-0176-x?r=1&l=ri&fst=0&error=cookies_not_supported&code=20def7ff-647e-4b3f-923a-66c0a437f01b
17 Hossmann, K.-A., & Hermann, D. M. (2002). Effects of electromagnetic radiation of mobile phones on the Central Nervous System. Bioelectromagnetics, 24(1), 49–62. https://doi.org/10.1002/bem.10068
18 Mheidly, N., Fares, M. Y., & Fares, J. (2020). Coping with stress and burnout associated with telecommunication and online learning. Frontiers in public health. Retrieved from https://www.frontiersin.org/articles/10.3389/fpubh.2020.574969/full
19 Pascoe, M. C., & Bauer, I. E. (2015). A systematic review of randomised control trials on the effects of yoga on stress measures and mood. Journal of Psychiatric Research, 68, 270–282. https://doi.org/10.1016/j.jpsychires.2015.07.013
20 Büssing, A., Michalsen, A., Khalsa, S. B., Telles, S., & Sherman, K. J. (2012). Effects of yoga on mental and physical health: A short summary of reviews. Evidence-Based Complementary and Alternative Medicine, 2012, 1–7. https://doi.org/10.1155/2012/165410
21 Fares, J., & Fares, Y. (2016). The role of yoga in relieving medical student anxiety and stress. North American Journal of Medical Sciences, 8(4), 202. https://doi.org/10.4103/1947-2714.179963
22 Heng, Y. T., & Schabram, K. (2021). Your Burnout is unique. your recovery will be, too. Harvard Business Review. Retrieved from https://hbr.org/2021/04/your-burnout-is-unique-your-recovery-will-be-too
23 Kirby, J. N. (2016). Compassion interventions: The programmes, the evidence, and implications for research and Practice. British Psychological Society. Retrieved from https://bpspsychub.onlinelibrary.wiley.com/doi/abs/10.1111/papt.12104
24 Weng, H., Fox, A., Shackman, A., Stodola, D., Caldwell, J., Olson, M., Rogers, G., & Davidson, R. (2013). Compassion training alters altruism and neural responses to suffering - journals.sagepub.com. Psychological Science. Retrieved from https://journals.sagepub.com/doi/abs/10.1177/0956797612469537?cited-by=yesl0956797612469537v1p0956797612469537v1r0956797612469537v1